Advanced Orthopedic Specialists is now offering one of the most comprehensive arthritis programs in the country. We now offer cutting edge therapies including surgical and non-surgical options to fit any lifestyle and severity of symptoms. We can provide a customized therapy program tailored to your specific symptoms and conditions as well as your active lifestyle. Just like no one drug is for every patient, no single cell based therapy is for every arthritic knee, hip, or shoulder. We offer a comprehensive program with multiple state of the art therapies to match each patient's condition as well as the specific lifestyle demands. Call 810-299-8550 for an appointment today.
Knee Arthroscopy Stem Cell Therapy by Laith Farjo, M.D.
Watch as Dr. Laith Farjo discusses what stem cell therapy is, and how it is incorporated into an actual knee arthroscopy surgery.
How Do Stem Cells Work?
By: Advanced Orthopedic Specialists - Brighton, MI
This is a very common question asked not only by our patients, but also many educated physicians using this therapy. After years and years of trying to understand this process myself, I have attempted to simplify this very complex and complicated system down to 3 easy to remember mechanisms. The problem with simplifying a complex system is that it can leave out some other minor systems at work, but if we want to take a 10,000 foot look at this mountain of information, I believe that you can begin to make more sense of this process by boiling this down to a few basic mechanisms. The goal is not to make anyone an expert, but rather just an informed consumer so you can make an educated and knowledgeable decision if this therapy may be a viable treatment for either yourself or your loved ones. Many great philosophers in the past such as Camus, Kierkegaard and Aristotle have suggested we narrow down complex systems into three reasons, examples or theories because it allowed the student to understand the subject in a coherent manner. Thus, I am following their suggestion to narrow this down to 3 main mechanisms.
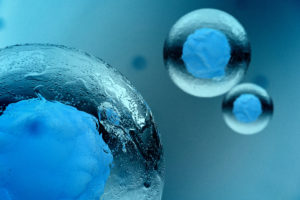
Before we talk about stem cells, we need to clarify that common stem cell therapies used in the United States contain a very small number of stem cells. Many treatment centers may only transfer a few thousand cells and thus, the mechanisms of action of these treatments are not due solely to the stem cells. Rather, they are due to the other nurturing biochemical compounds found around these cells. Therefore, bone marrow is very important in this process. Bone marrow is the natural home environment for stem cells in your body. This is where they are born, raised and utilized. Thus, we need to consider the contributions of the bone marrow products surrounding the stem cells such as Interleukin 1-B receptor antagonist (that was a mouthful) and Alpha 2 Macroglobulin as well as Transforming Growth Factor- Beta. These are important to help set the proper environment for stem cells to conduct their work. So, the title of this section is a bit misleading and should say “How does Cell Therapy Work?”
So, what are these three mechanisms of action? They are very easy to remember since they all start with R. This is what we call a pneumonic because they sound similar and are easier to remember. These mechanisms are:
Reduce
Restore
Regenerate
We will take each one and explain how this mechanism relates to cell based therapies.
Reduce- Cell based therapies reduce the harmful biochemical storm in your joint. We normally have nice balance of specific biochemicals in our joints. They serve to help maintain the normal cell function of the joint. However, as we age, or with trauma or with specific inflammatory diseases of the joint, this chemical balance is upset and we have too many pro-inflammatory chemicals causing continued destruction. One of the most important biochemical families are the interleukins and especially interleukin-1-beta. This is normally used to help regulate our response to infection or inflammation. However, the production of this biochemical begins to rise and cause widespread inflammation and destruction of both cartilage and bone. Interleukin 1-B is the “Kingpin” or “Godfather” of these biochemicals and REDUCING IL-1 B will help restore this normal balance. Many biochemical pathways lead back to Interleukin-1 B and just like the Corleone family, when we start to investigate who is causing all this crime and destruction, many pathways lead back to the “Godfather” biochemical. Interleukin-1B controls the judges, the newspapers, and the police in New York City just like Don Corleone.
How is this done? Our own bone marrow contains a natural inhibitor of IL-1 B called Interleukin 1-B receptor antagonist. This is the antidote for the toxic effects of IL-1B and it is found intimately wrapped in the environment of your stem cells throughout your bone marrow. When we take your own bone marrow, there is a nice concentration of this natural inhibitor already present and connected to your stem cells. Race horses have used Interleukin 1-B Receptor Antagonist for the past 12 years to treat arthritis and improve their performance. In fact, this therapy is so effective and popular, one horses in the 2017 Kentucky Derby was named IRAP which stands for the IL-1 B receptor antagonist. As humans, you only require a small amount of interleukin-1 B receptor antagonist in a ratio of 100:1 for it to be effective in REDUCING its activity.
Thus, Bone Marrow Concentrate taken from your own pelvis can REDUCE the biochemical storm happening in your joint naturally and effectively. Without this reduction, there is little hope that any cartilage cells will survive and continued destruction will occur.
Our next mechanism involves Restoring the normal cell to cell communication of a joint.
Your joint is an organ just like a kidney, brain or heart. An organ is a group of specialized cells working together to perform a specific function. For example, your kidney cells function together to filter out toxins in your blood and help maintain healthy blood pressure. Your joint has specific cells designed to allow smooth and efficient movement of your body. To accomplish this goal, the specialized cells need to talk to one another through a special communication mechanism for one cell to talk to another local cell. This is called paracrine signaling. A diseased joint has a dysfunction of this signaling due to guess who….”The Godfather.” In a normal joint, cartilage cells need to talk to other cartilage cells to help with their normal function. Bone cells need to talk to other bone cells to do the same. When Interleukin 1-B is elevated, tunneling through the diseased bone next to your joint occurs and bone cells start to talk to cartilage cells rather than other bone cells through a mechanism called “cross talk”.
This cross talk is just like someone trying to give you directions to a restaurant when everyone else is talking very loudly in the background. Both parties on the line become frustrated and eventually hang up. Your bone and cartilage cells do the same and become dysfunctional unable to perform the specialized functions they were born to do because they cannot communicate effectively with each other. The bone marrow concentration helps RESTORE this normal cell to cell signaling by reducing the Interleukin-1 B and shutting down the tunnels between bone and cartilage. Over time, the small tunnels are shut down and cartilage cells now talk only to cartilage cells so they can function like a normal organ. Normal tissue function returns which in turn RESTORES the normal function of the joint as an organ.
Finally, we can discuss Regenerate as the third, but least important mechanism of cell therapy. Although many so called stem cell clinics claim the regenerative properties of their therapy is the most important mechanism, as we can see from the two previous mechanisms, unless you have a stable environment first, there is no reason to regenerate any tissue because it will be either destroyed by the biochemical storm caused by the Godfather or if by some miracle, there is tissue growth, the cells won’t be able to function as a normal organ because of the loss of paracrine signaling or cell to cell communication. So, cell based therapies REDUCE this biochemical imbalance and RESTORE normal cell to cell communication setting the stage for proper REGENERATION.
Think about this process compared to another very common disease in our country. Alcoholism is very prevalent in our society. I don’t really need to remind anyone of it’s prevalence. Ironically, just about the same number of people in the United States are affected by Arthritis as Alcoholism which is about 28 million. If we look at one of the most effective treatments for alcoholism, we can see a parallel to the three mechanisms of cell based therapies. Alcohol recovery programs normally begin with the removal of the harmful chemicals, or alcohol, causing the problem. In cell based therapies, we remove the harmful biochemical causing continued destruction. Without the removal of alcohol, the destructive process continues and this is the same for your joint. Next, critical relationships are restored through personal, family and marriage counseling. During counseling, broken lines of communication are restored.
In cell based therapy, broken and dysfunctional cell to cell communication is restored. Once the harmful chemical has been REDUCED and the communication RESTORED, now the family can thrive and function again and grow in a stable, non-toxic and loving environment. Your joint is the same with the REDUCED toxic chemicals and in a stable RESTORED environment promoting the REGENERATION of new tissue. The amount of new tissue may be very small in relation to the dramatic effects of reducing the toxins and restoring the normal function of the cells, but it is still a property of the mesenchymal stem cells delivered in the bone marrow concentrate. There is little relationship between the amount of tissue regenerated and the relief of your pain. However, there is a direct and linear relationship between levels of Interleukin-1 beta and the severity of your arthritic symptoms. Thus, reducing this harmful biochemical is paramount to the restoration and regeneration of your joint.
To prove this point, think of the last time you took a pill for your arthritis pain. Not everyone responds to these pills, but most people have some relief for a brief period of time after taking such a medication. Pills such as Aleve or Motrin have absolutely no effect on regenerating new cartilage tissue. Yet, you may have experienced some relief for about 4 to 6 hrs. Have you ever wondered how this happened? From a biochemical perspective, this medication reduced one of the biochemical pathways causing pain in your joint. Yet, this is pill in your stomach and not in your joint and it did not regenerate any new tissue and may have contributed to some further tissue destruction, but it provided some relief! Bone marrow concentrate stem cell therapy provides long term REDUCTION of the most important “Godfather” biochemical pathways for years and it RESTORES normal cell to cell communication leading to an optimal environment for the icing on the cake which is REGENERATION of some tissue.
I hope this simple explanation has accomplished its goal of making you a more informed and educated consumer and hopefully you can now understand if this therapy may be helpful for your our your loved one’s joint. The use of cell therapy can help your body naturally reduce a harmful chemical imbalance; restore cell to cell communication; and regenerate new tissue all adding up to a joint with lower pain and higher function without side effects or the inconvenience and risk of major surgery.
Safe, Effective and FDA Allowed Cell Therapy at AOS
Recent news articles in the Wall Street Journal and radio and TV reports of FDA issuing warnings to illegal stem cell clinics have generated a well deserved concern from the public and the media regarding unfounded and potentially unsafe stem cell treatments in the United States. The warnings were issued to unscrupulous and unregulated stem cell clinics in California and Florida. These stem cell therapies have nothing to do with the current therapies available at Advanced Orthopedic Specialists. We are, and always have been compliant with the FDA definitions of regulated cells. This is why we only offer bone marrow derived products as outlined by the FDA Code of Federal Regulations, Title 21, Volume 8 and recently revised as of April 1, 2017. Within this code under section 1271.3, paragraph D and section 4, bone marrow is permitted for use of cellular products. This ruling can be reviewed by clicking onto: FDA Ruling. Thus, our goal of providing safe, effective, ethical therapy to our patients is within full compliance with the FDA. We have been extremely careful and cautious in offering these therapies only to patients who may benefit from these treatments and have tried to provide the safest and most effective protocols to ensure the safe harvesting, processing and delivery of this therapy. We make no wild claims and only treat conditions that may benefit from this therapy. The result is a treatment where over 82.5% of our patients improve with most receiving over 50% improvements from baseline. This still means there are some patients who do not respond, and we try our hardest to identify these patients and recommend another form of treatment. However, we strive to provide all of our patients with the safest, most effective and compliant therapies. As we continue to improve these therapies, we are hopeful that this will provide relief to our patients suffering from bone and joint disease. But, we will always do this in a safe and compliant manner.
New Study Proves Benefits of Bone Marrow Stem Cells for Knee Arthritis
By: Edward G. Loniewski, DO, FACOS, FAOAO
A very recent publication in the International Journal of Rheumatic Diseases (Int J Rheum Dis. 2017 Jul 27. doi: 10.1111/1756-185X.13139) revealed that a single dose injection of bone marrow stem cells taken from the pelvis provided statistically significant improvement in function and reduction of pain which continued to improve in greater degrees as time progressed. This was a controlled study meaning that it was compared to a similar group of patients who received another commonly accepted treatment for arthritis and in this study it was compared to acetaminophen otherwise known as Tylenol. What was interesting was the fact that the patients who received the stem cell injection into their knee had improvements in their ability to complete normal activities of daily living such as dressing; exiting a car; shopping and bathing at each measurement point and the differences continued to improve as the study progressed. Thus, a difference was noted early in the study and this difference improved more and more as the study went forward. This response is unlike many other treatments provided in medicine especially when it relates to pain relief. Most of the medications or treatments we provide have a "leveling off" effect, but this treatment seems to have a "progressive " effect. The differences in the two groups started very early at 1 week after treatment and continued to improve at 1 month and 6 months after the treatment. Some of the criticisms of this study is that 6 months is still considered to be short term , and there was a lack of reporting how many of the patients did not respond. In addition, this was not a blinded or placebo controlled meaning that both the patient and the physician or researcher knew who received which treatment. Furthermore, this study utilized a pre-treatment drug designed to stimulate stem cells to move from the bone marrow into the bloodstream. This is known as a Granulocyte Colony Stimulating Factor (G-CSF) sold under the trade name Biofilgran. This same medication is used when a stem cell transplant is used for certain blood born cancers. The patients in this study who received this treatment prior to the stem cell harvest tolerated the treatment well with only some minor and temporary bone pain. Despite some of these criticisms, this study is an honest attempt to demonstrate that a simple treatment of stem cells and bone marrow taken from the same patient can provide statistically significant superior relief of pain and an improvement compared to the use of acetaminophen. This effect continues to improve over a prolonged period of time. Every month, new studies like this one helps justify the use of your own stem cells to help you recover from the pain and disability of arthritis. If you would like to read this study yourself, you can find this at: STEM CELL STUDY
Advanced Orthopedic Specialists offer a similar treatment and Dr. Loniewski is offering a pre and post treatment protocol designed to improve your results. We have the most experience providing these treatments than any other stem cell group in the State of Michigan and have been providing cell based therapy to our patients since 2005. We only offer this to patients who fit specific criteria since no single treatment provides optimal results for every patient. Our goal is to provide you with the best treatment for your condition because not all patients are candidates for cell based therapies. To find out if you may be a candidate please download our stem cell questionnaire at: AM I A CANDIDATE FOR CELL THERAPY
and call our office at 810-299-8550 for a comprehensive evaluation.
Stem Cell Newsletter
By: Edward G. Loniewski, DO, FACOS, FAOAO
Advanced Orthopedic Specialists was the first orthopedic office to offer stem cell therapy to patients in Michigan. We have always attempted to provide the highest quality, cutting edge technology to our patients in an ethical and effective manner. We have patients coming from all over the country to have this treatment done right here in Brighton, Michigan. Thus, we have developed a cutting edge newsletter to keep you informed on the latest developments in cell based therapies as well as providing you with practical tips on how to maximize the benefits of cell therapy. The newsletter will contain short, to the point articles on:
Latest updates on stem cell therapy
Brief reviews of stem cell research
Tips on exercise
Local chefs' share cell friendly recipes
Patient stories
Frequently asked questions from Dr. Edward Loniewski
If you are interested in receiving this first of it's kind newsletter, just click on the link below.
Simple Exercise Improves Stem Cell Therapy
20 minutes a day can make a difference
Simple cyclic low stress exercise for only 20 minutes per day helped improve the results of stem cell therapy. Researchers at the Sapporo University School of Medicine in Japan and Yale University have found that adding simple walking exercises to rats who received mesenchymal stem cells for a chemically induced stroke not only significantly reduced the size of the stroke lesion in the brain but also stimulated more brain activity and improved their ability to recover from the stroke compared to rats who received stem cell therapy alone. Another study conducted at the Yamaguchi School of Medicine found that simple eccentric muscle exercises of your thigh muscles such as performing wall squats activated stem cell proliferation for up to 5 days after the exercise. So, it does appear that we may be able to improve the number of stem cells activated and the overall results of stem cell therapy with simple, motion and stretching exercises. We encourage our patients to participate in a 20 minute per day exercise program such as 15 minutes of stationary bike riding and 5 minutes of thigh muscle exercises. Advanced Orthopedic Specialists offers one on one therapy with a registered and certified physical therapist if they prefer a more personalized instruction.
Synergic Effects of Rehabilitation and Intravenous Infusion of Mesenchymal Stem Cells After Stroke in Rats. Sasaki Y, Sasaki M, Kataoka-Sasaki Y, Nakazaki M, Nagahama H, Suzuki J, Tateyama D, Oka S, Namioka T, Namioka A, Onodera R, Mikami T, Wanibuchi M, Kakizawa M, Ishiai S, Kocsis JD, Honmou O. Phys Ther. 2016 Nov;96(11):1791-1798. Epub 2016 May 12.
Effect of eccentric contraction on satellite cell activation in human vastus lateralis muscle.
Imaoka Y, Kawai M, Mori F, Miyata H. J Physiol Sci. 2015 Sep;65(5):461-9. doi: 10.1007/s12576-015-0385-4. Epub 2015 Jun 27.
How Do Stem Cells Work?
How Do Stem Cells Work?
By: Edward G. Loniewski, DO, FACOS, FAOAO
This is a very common question asked not only by our patients, but also many educated physicians using this therapy. After years and years of trying to understand this process myself, I have attempted to simplify this very complex and complicated system down to 3 easy to remember mechanisms. The problem with simplifying a complex system is that it can leave out some other minor systems at work, but if we want to take a 10,000 foot look at this mountain of information, I believe that you can begin to make more sense of this process by boiling this down to a few basic mechanisms. The goal is not to make anyone an expert, but rather just an informed consumer so you can make an educated and knowledgeable decision if this therapy may be a viable treatment for either yourself or your loved ones. Many great philosophers in the past such as Camus, Kierkegaard and Aristotle have suggested we narrow down complex systems into three reasons, examples or theories because it allowed the student to understand the subject in a coherent manner. Thus, I am following their suggestion to narrow this down to 3 main mechanisms. But I think a more important reason is that I can’t remember more than three things at a time!
Before we talk about stem cells, we need to clarify that common stem cell therapies used in the United States contain a very small number of stem cells. Many treatment centers may only transfer a few thousand cells and thus, the mechanisms of action of these treatments are not due solely to the stem cells. Rather, they are due to the other nurturing biochemical compounds found around these cells. Therefore, bone marrow is very important in this process. Bone marrow is the natural home environment for stem cells in your body. This is where they are born, raised and utilized. Thus, we need to consider the contributions of the bone marrow products surrounding the stem cells such as Interleukin 1-B receptor antagonist (that was a mouthful) and Alpha 2 Macroglobulin as well as Transforming Growth Factor- Beta. These are important to help set the proper environment for stem cells to conduct their work. So, the title of this section is a bit misleading and should say “How does Cell Therapy Work?”
So, what are these three mechanisms of action? They are very easy to remember since they all start with R. This is what we call a pneumonic because they sound similar and are easier to remember. These mechanisms are:
Reduce
Restore
Regenerate
We will take each one and explain how this mechanism relates to cell based therapies.
Reduce- Cell based therapies reduce the harmful biochemical storm in your joint. We normally have nice balance of specific biochemicals in our joints. They serve to help maintain the normal cell function of the joint. However, as we age, or with trauma or with specific inflammatory diseases of the joint, this chemical balance is upset and we have too many pro-inflammatory chemicals causing continued destruction. One of the most important biochemical families are the interleukins and especially interleukin-1-beta. This is normally used to help regulate our response to infection or inflammation. However, the production of this biochemical begins to rise and cause widespread inflammation and destruction of both cartilage and bone. Interleukin 1-B is the “Kingpin” or “Godfather” of these biochemicals and REDUCING IL-1 B will help restore this normal balance. Many biochemical pathways lead back to Interleukin-1 B and just like the Corleone family, when we start to investigate who is causing all this crime and destruction, many pathways lead back to the “Godfather” biochemical. Interleukin-1B controls the judges, the newspapers, and the police in New York City just like Don Corleone.
How is this done? Our own bone marrow contains a natural inhibitor of IL-1 B called Interleukin 1-B receptor antagonist. This is the antidote for the toxic effects of IL-1B and it is found intimately wrapped in the environment of your stem cells throughout your bone marrow. When we take your own bone marrow, there is a nice concentration of this natural inhibitor already present and connected to your stem cells. Race horses have used Interleukin 1-B Receptor Antagonist for the past 12 years to treat arthritis and improve their performance. In fact, this therapy is so effective and popular, one horses in the 2017 Kentucky Derby was named IRAP which stands for the IL-1 B receptor antagonist. As humans, you only require a small amount of interleukin-1 B receptor antagonist in a ratio of 100:1 for it to be effective in REDUCING its activity.
Thus, Bone Marrow Concentrate taken from your own pelvis can REDUCE the biochemical storm happening in your joint naturally and effectively. Without this reduction, there is little hope that any cartilage cells will survive and continued destruction will occur.
Our next mechanism involves Restoring the normal cell to cell communication of a joint.
Your joint is an organ just like a kidney, brain or heart. An organ is a group of specialized cells working together to perform a specific function. For example, your kidney cells function together to filter out toxins in your blood and help maintain healthy blood pressure. Your joint has specific cells designed to allow smooth and efficient movement of your body. To accomplish this goal, the specialized cells need to talk to one another through a special communication mechanism for one cell to talk to another local cell. This is called paracrine signaling. A diseased joint has a dysfunction of this signaling due to guess who….”The Godfather.” In a normal joint, cartilage cells need to talk to other cartilage cells to help with their normal function. Bone cells need to talk to other bone cells to do the same. When Interleukin 1-B is elevated, tunneling through the diseased bone next to your joint occurs and bone cells start to talk to cartilage cells rather than other bone cells through a mechanism called “cross talk”.
This cross talk is just like someone trying to give you directions to a restaurant when everyone else is talking very loudly in the background. Both parties on the line become frustrated and eventually hang up. Your bone and cartilage cells do the same and become dysfunctional unable to perform the specialized functions they were born to do because they cannot communicate effectively with each other. The bone marrow concentration helps RESTORE this normal cell to cell signaling by reducing the Interleukin-1 B and shutting down the tunnels between bone and cartilage. Over time, the small tunnels are shut down and cartilage cells now talk only to cartilage cells so they can function like a normal organ. Normal tissue function returns which in turn RESTORES the normal function of the joint as an organ.
Finally, we can discuss Regenerate as the third, but least important mechanism of cell therapy. Although many so called stem cell clinics claim the regenerative properties of their therapy is the most important mechanism, as we can see from the two previous mechanisms, unless you have a stable environment first, there is no reason to regenerate any tissue because it will be either destroyed by the biochemical storm caused by the Godfather or if by some miracle, there is tissue growth, the cells won’t be able to function as a normal organ because of the loss of paracrine signaling or cell to cell communication. So, cell based therapies REDUCE this biochemical imbalance and RESTORE normal cell to cell communication setting the stage for proper REGENERATION.
Think about this process compared to another very common disease in our country. Alcoholism is very prevalent in our society. I don’t really need to remind anyone of it’s prevalence. Ironically, just about the same number of people in the United States are affected by Arthritis as Alcoholism which is about 28 million. If we look at one of the most effective treatments for alcoholism, we can see a parallel to the three mechanisms of cell based therapies. Alcohol recovery programs normally begin with the removal of the harmful chemicals, or alcohol, causing the problem. In cell based therapies, we remove the harmful biochemical causing continued destruction. Without the removal of alcohol, the destructive process continues and this is the same for your joint. Next, critical relationships are restored through personal, family and marriage counseling. During counseling, broken lines of communication are restored.
In cell based therapy, broken and dysfunctional cell to cell communication is restored. Once the harmful chemical has been REDUCED and the communication RESTORED, now the family can thrive and function again and grow in a stable, non-toxic and loving environment. Your joint is the same with the REDUCED toxic chemicals and in a stable RESTORED environment promoting the REGENERATION of new tissue. The amount of new tissue may be very small in relation to the dramatic effects of reducing the toxins and restoring the normal function of the cells, but it is still a property of the mesenchymal stem cells delivered in the bone marrow concentrate. There is little relationship between the amount of tissue regenerated and the relief of your pain. However, there is a direct and linear relationship between levels of Interleukin-1 beta and the severity of your arthritic symptoms. Thus, reducing this harmful biochemical is paramount to the restoration and regeneration of your joint.
To prove this point, think of the last time you took a pill for your arthritis pain. Not everyone responds to these pills, but most people have some relief for a brief period of time after taking such a medication. Pills such as Aleve or Motrin have absolutely no effect on regenerating new cartilage tissue. Yet, you may have experienced some relief for about 4 to 6 hrs. Have you ever wondered how this happened? From a biochemical perspective, this medication reduced one of the biochemical pathways causing pain in your joint. Yet, this is pill in your stomach and not in your joint and it did not regenerate any new tissue and may have contributed to some further tissue destruction, but it provided some relief! Bone marrow concentrate stem cell therapy provides long term REDUCTION of the most important “Godfather” biochemical pathways for years and it RESTORES normal cell to cell communication leading to an optimal environment for the icing on the cake which is REGENERATION of some tissue.
I hope this simple explanation has accomplished its goal of making you a more informed and educated consumer and hopefully you can now understand if this therapy may be helpful for your our your loved one’s joint. The use of cell therapy can help your body naturally reduce a harmful chemical imbalance; restore cell to cell communication; and regenerate new tissue all adding up to a joint with lower pain and higher function without side effects or the inconvenience and risk of major surgery.
Reduce, Restore and Regenerate are the 3 R's of Stem Cell Therapy
Reduce Biochemical Imbalances; Restore Cell to Cell Communication and Regenerate New Tissue by: Edward G. Loniewski, DO, FACOS, FAOAO
A very common question asked by many patients and even well informed and educated doctors is how cell based therapies such as bone marrow derived stem cells may work. After years of researching and understanding this technology, we can reduce this answer to three simple steps. Although we could give you more than a hundred mechanisms, we chose three since most people can remember 3 steps. If we have more than three, everyone in our multitasking and attention deficit infused society begins to forget numbers one and two. Many philosophers such as Camus, Kierkegaard or even Aristotle suggest we narrow down our explanations of complex thought and systems down to three reasons, examples or theories. Following in this tradition, we can help simplify this very complex field of healthcare down to three major mechanisms of action for cell based therapies. These are;
Reduce
Restore
Regenerate
Reduce- Cell based therapies help restore the natural biochemical balance. We normally have a complex set of biochemical byproducts of cellular maintenance in our joints. When this is in normal balance, it is called homeostasis. However, as we age, or when trauma or disease occurs in a joint, this balance is interrupted and mass destruction and pain occur. One of the most important biochemical markers is Interleukin 1-Beta ( IL-1 B) . Although this Interleukin is normally used to clean up cellular debris, arthritic joints produce too much, causing the destruction of the repair. Each time our body tries to repair itself, this abnormally high amount of Interleukin 1- Beta disrupts this process. At Advanced Orthopedic Specialists, we can produce a bone marrow derived product from your own cells to naturally reduce the abnormally high levels of the IL-B. We can filter and concentrate of a natural blocker found in everyone's own bone marrow called Interleukin 1- Beta Receptor Antagonist ( IL-1B Ra) . Your own body produces this within your bone marrow and in smaller amounts in your blood. We have found a way to concentrate this through a patented filtering process producing over 4 times the concentration found in any other preparation. Without this important step, it is very difficult for your joint to restore its natural biochemical balance or homeostasis.
Restore - Your joint is an organ just like your brain, kidney, liver or heart. An organ is made up of cells which perform a specific function necessary for life. These cells carry on their purpose by communicating efficiently between each other. This is called cell-to-cell communication or a paracrine signaling. When an organ such as your knee has arthritis, the cells begin to act abnormal and the communication between these cells breaks down. The result is a dysfunctional joint. This is what happens in a dysfunctional family. Nobody communicates effectively with each other and the family unit begins to break down. However, Mesenchymal Stem Cells (MSC's) can restore normal paracrine signaling of cells through the release of specific factors designed to restore function of the joint. Thus, when stem cells restore this normal communication, the normal functions of the joint return. A patented processing technology coupled with a significantly improved cell harvest technique can improve cell harvesting by over 345% and return of more than 90% of your cells back to your body. This provides the absolute highest number of mesenchymal stem cells to your joint to ensure that your normal cell to cell communication is restored.
Regenerate- Only after a joint has completed the first two steps of this process, can we move forward with the building of new tissue or regeneration. After we have reduced the levels of harmful biochemical byproducts in your joints to a reasonable or near normal level, and after restoring cell to cell communication, your joint may now begin the process of producing new tissue. Think about this scenario like a family with an alcoholic father. There is nothing like alcoholism as a source of family dysfunction. In fact. there are just about the same number of children with alcoholic parents as there are people with arthritis (about 28 million) in the United States. If this family is to survive, the first step is to reduce the chemical causing the destruction. In the family, this is alcohol. In the joint, this is Interleukin-1- Beta. The second step is to encourage the family to communicate and re-establish the lines of normal communication. In the family suffering from alcoholism, this is called therapy and in the joint this is called a paracrine event. Once the chemical in the family is reduced and the communication is restored, regeneration will be able to occur and the family will be able to function as a normal family and the children will be able to thrive. In the joint, we have reduced the harmful biochemical imbalance and restored cell to cell communication and new tissue can now regenerate. However, the actual amount of tissue needed for pain relief may be very minimal. There is no relationship between the amount or volume of new tissue formation and the level of pain relief or the restoration of joint function. Some people can produce very large amounts of new tissue and have very little change in their pain or function. However, many patients may have very little, if any, tissue regeneration and have significant pain relief and restoration of function. Why would this be true? Think about the last time you had joint pain and you took a simple over the counter medication to relieve this pain. Most people would have a reduction of their pain. However, this pain reliever did not grow any new tissue by any means. These medications are not injected into your joint, and your stomach does not directly connect to your joint. However, whenever you take a pill, your joint has a good chance that it will feel better and allow you to function at a higher level. Why is this true? The answer is the fact that these medications help to temporarily reduce some other minor players in the biochemical imbalance of your joint. Thus, new tissue is not necessary to reduce the pain and restores some of the function to your joint. Mesenchymal stem cells do this, but through a much more complex system and for a substantially longer period with a positive side effect of possibly growing more tissue.
The use of cell therapy can help your body naturally reduce a harmful chemical imbalance; restore cell to cell communication; and regenerate new tissue all adding up to a joint with lower pain and higher function without side effects or the inconvenience and risk of major surgery.
Concentrating Stem Cell Therapy Naturally
Concentrating Stem Cell Therapy Naturally
By : Edward G. Loniewski, DO, FACOS, FAOAO
At Advanced Orthopedic Specialists we strive to provide you with cutting edge technology sometimes not even available at such stalwarts of medical innovation such as John Hopkins; The Mayo Clinic or even the University of Michigan. One of these advanced technologies involves the concept of concentrating the healing cells from your bone marrow or blood in the joint or area of damage. The simple filtering of your bone marrow or blood plasma to remove water and salts helps to naturally concentrate the important plasma proteins and growth factors found in this vital fluid found within each and every human. In the past, stem cell therapy involved spinning your bone marrow or blood at very high speeds to separate it into two to three different layers, namely the red blood cell layer, the platelet poor plasma (PPP) layer; and a platelet/ stem cell rich plasma ( PRP) layer.
In the past, many researchers or physicians would discard both the red blood cell layer and the platelet poor plasma (PPP) layer. However, this never really made sense to me since this PPP layer contains many of the growth factors and plasma proteins necessary for continued growth of these cells. In fact, one of the best growth mediums for mesenchymal stem cells is a special mixture called platelet lysate made from the layer we would normally throw away in the biohazard bag. The problem using this PPP layer in the past is that it would dilute the mesenchymal stem cells as well as the concentrated platelets we need to activate in your body by forming a clump or a clot. However, some very smart and practical scientists at Celling Biosciences (Austin, Tx.) used good old fashioned American ingenuity to figure out a simple filtering process which can easily remove water and salts from this PPP to produce a super clot forming; growth factor and plasma protein rich environment for harvested stem cells. The concept is extremely simple and safe using no drugs or chemicals. This filtering process is a patented technology only available through a US born and bred company in Austin, Texas. Celling Bioscience's PhD's have used this self contained filter to significantly enhance the retention and growth of stem cells within your joints. In fact, they have demonstrated that this technology can increase the concentration of very vital growth factors such as Alpha 2 Macroglobulin (A2M) by a factor of 5.22 , Platelet Derived Growth Factor (PDGF-bb) by a factor of 5.88 , Vascular Endothelial Growth Factor (VEGF) by a factor of 2.27 as well as the very important Interleukin 1 Receptor Antagonist Protein (IRAP) by over 3.77 times the normal amount. In addition, this concentrating process helps the cells clump in a manner to protect them from migration to other parts of your body and slowly release themselves over a prolonged period of time. If there is no clumping of these cells within the area of delivery such as within your joint, you may rapidly lose these important cells within minutes.
Mesenchymal stem cells have a high affinity to blood vessels and travel to your spleen, lymph or circulatory system and away from the area of damage. Sometimes, stem cell clinics or researchers use artificial clotting agents such as human recombinant (meaning made from DNA taken from another human) or bovine (meaning from horses) thrombin to create this clot. The problem is that a percentage of patients react to this drug, and repetitive use of this drug can have an autoimmune response causing pain and swelling and possible cell death. On the other hand, you should never develop a reaction to a concentrate of your own cells. In a recent, trial conducted at Celling Biosciences, Matthew Murphy, PhD. was able to demonstrate that the super healthy clot formed from the concentrated plasma proteins allowed the clot to continue to hold it's shape for an amazing 14 days with very high cell counts. On the other hand, the clot formed by the drug thrombin had started to deteriorate only after 6 days with a much lower cell count. Dr. Loniewski, has worked with Celling Biosciences to help develop state of the art protocols using this technology and the most advanced stem cell therapies. No other center in the United States offers this advanced technology on all of their patients. This is why we can claim that at least 85% of our patients improve with little to no side effects. Not all patients respond to these treatments, and not every patient is a candidate for cell based therapies. If you are interested in cell based treatments, call our office at 810-299-8550 or you can download our on-line stem cell questionnaire to understand if you may be a candidate for this therapy.


 This cross talk is just like someone trying to give you directions to a restaurant when everyone else is talking very loudly in the background. Both parties on the line become frustrated and eventually hang up. Your bone and cartilage cells do the same and become dysfunctional unable to perform the specialized functions they were born to do because they cannot communicate effectively with each other. The bone marrow concentration helps RESTORE this normal cell to cell signaling by reducing the Interleukin-1 B and shutting down the tunnels between bone and cartilage. Over time, the small tunnels are shut down and cartilage cells now talk only to cartilage cells so they can function like a normal organ. Normal tissue function returns which in turn RESTORES the normal function of the joint as an organ.
This cross talk is just like someone trying to give you directions to a restaurant when everyone else is talking very loudly in the background. Both parties on the line become frustrated and eventually hang up. Your bone and cartilage cells do the same and become dysfunctional unable to perform the specialized functions they were born to do because they cannot communicate effectively with each other. The bone marrow concentration helps RESTORE this normal cell to cell signaling by reducing the Interleukin-1 B and shutting down the tunnels between bone and cartilage. Over time, the small tunnels are shut down and cartilage cells now talk only to cartilage cells so they can function like a normal organ. Normal tissue function returns which in turn RESTORES the normal function of the joint as an organ.

 By: Edward G. Loniewski, DO, FACOS, FAOAO
By: Edward G. Loniewski, DO, FACOS, FAOAO